Mohammed El Sharkawy
Case Summary
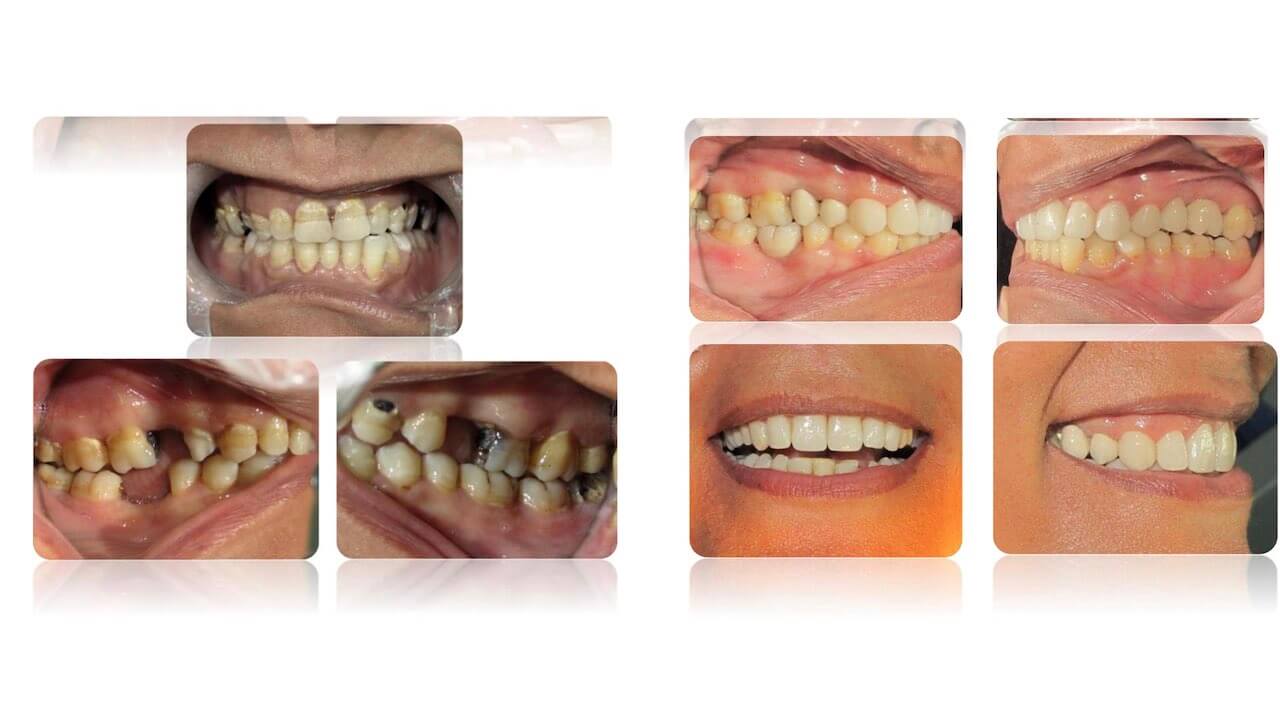
Patient H.F. presented with severe pain, she had multiple missing teeth restored with cantilever resin bonded bridges, a single crown and Porcelain laminate veneers for Smile rehabilitation.
PRE-TREATMENT ASSESSMENT
PATIENT DETAILS
-
Initials: H.F.
-
Sex: Female
-
Date of birth: 2nd of Dec 1977
-
Age at start of treatment: 38
-
Occupation: Super market CashierPATIENT CHIEF COMPLAINT
The patient pointed to her UR4 complaining from severe pain and pain on biting.
PATIENT OTHER COMPLAINTS
-
Recurrent pain and swelling in upper left area with Pain on biting on UL6.
-
Multiple missing teeth.
-
Patient doesn’t like her smile.HISTORY OF CHIEF COMPLAINT
Patient had a filling in that tooth many years ago, the filling was lost and the patient
didn’t go for further treatment in that tooth, tooth had episodes of pain lately but it
started to be severely painful 2 days ago.
HISTORY OF OTHER COMPLAINTS
-
The whole upper left area had swelling episodes for several months, The UL6 had a
filling about 5 years ago and it started being painful on biting since about a year.
-
Multiple extractions due to extensive caries and pain.
-
Linear discolored defect since childhood, no history of tooth chipping.RELEVANT MEDICAL HISTORY
- Patient is fit and well.
- No known allergies.
- No medications.
PAST DENTAL HISTORY
-
Rarely brush.
-
Doesn’t use any dental aids or mouth wash.
-
Irregular attendee.
-
Patient had some dental extractions and fillings.
-
Previous white fillings to cover discolored anterior teeth.SOCIAL HISTORY
-
Married.
-
Works as a cashier.
-
Doesn’t drink alcohol.
-
Doesn’t smoke or had previous history of smoking.CLINICAL EXAMINATION: EXTRA-ORAL FEATURES
-
Normal Extra-Oral features.
-
Normal TMJ articulation with no clicking or shifting.
-
Normal muscles of mastication.
-
Palpable left Submandibular lymph nodes.CLINICAL EXAMINATION: INTRA-ORAL FEATURES
Soft tissues:
- Red, swollen gingival tissues with loss of stippling and bleeding on probing.
- Thick gingival biotype.
- Other intra-oral soft tissues are considered normal. Bleeding index 64% Plaque index 69%

OCCLUSAL FEATURES
Static occlusion:
Incisor relationship:
-
Class I relationship
-
Cross bite in LL2Overjet: 2 mm
Overbite: 2 mmDynamic Occlusion:
Retruded contact position doesn’t coincide with intercuspal position.
Lateral excursion:
-
Right: Group function – UR3 with LR3 and LR4.
-
Left: Group function – LL3 and LL4 with UL3.
-
No working or Non-working side interferences.Protrusion:
Guided by anterior teeth with no posterior interference.
Cross-bite:
LL2 in cross bite with UL1 and UL2.
Critical Appraisal
Regardig the choice of restoration
Some sites with reduced alveolar ridge thickness and height (Seibert Class III ridge
resorption) precluded the use of implant supported restorations as a treatment,
implant placement in these sites would require vertical bone augmentation, a
procedure which is techniqually demanding with guarded prognosis (9), the
patient was also not motivated to go through this surgical procedure, RBB are
fixed minimally invasive restorations with high mediam term survival rate which
was a very good option for the patient.
Regarding bonding to Enamel
Linear enamel hypoplasia is characterised by linear enamel deffects, these
deffects are localized and doesn’t seem to affect bonding strength in the
otherwise normal enamel, palatal enamel of posteriors was noticed to be clear of
any hypoplastic lesions.
Regarding choice of veneering material
Choice of restoration type should be made on individual patient basis, taking into
account patient preference, as composite veneers have more surface quality
changes, and although there is no clear evidence to support any treatment option
over the other in terms of durability (10,11), this was explained to the patient. As
she tried tooth colored restorations during early age but they were not durable
and failed she favoured using another durable and color stable option in the
esthetic rehabilitation procedures.
References
(1) Chen E, Abbott PV. Evaluation of Accuracy, Reliability, and Repeatability of Five Dental Pulp Tests. J
Endod 2011;37:1619–1623
(2) Weiger, R., Rosendahl, R. and Löst, C. (2000), Influence of calcium hydroxide intracanal dressings on
the prognosis of teeth with endodontically induced periapical lesions. International Endodontic Journal,
33: 219–226
(3) Quirynen, M., De Soete, M., Boschmans, G., Pauwels, M., Coucke, W., Teughels, W. and Van
Steenberghe, D. (2006), Benefit of “one-stage full-mouth disinfection” is explained by disinfection and root
planing within 24 hours: a randomized controlled trial. Journal of Clinical Periodontology, 33: 639–647
(4) Poyato Ferrera M, Segura-Egea JJ, Bullon-Fernandez P. Comparison of modified bass technique with
normal tooth brushing practices for efficacy in supragingival plaque removal. Int. J Dent Hygiene 2003;
110:114
(5) Roe L, Hunt P, Bradshaw H, Rayner M. Health promotion interventions to promote healthy eating in
the general population: a review. London: Health Education Authority. Health Promotion Effectiveness
Reviews; 6. 1997
(6) Pjetursson et al. A systematic review of the survival and complication rates of resin-bonded bridges
after an observation period of at least 5 years.
(7) Rashid S A, Al-Wahadni A M, Hussey D L. The periodontal response to cantilevered resin-bonded
bridgework. J Oral Rehabil 1999; 26: 912–917
(8) Ferrari M. et al. Post placement affects survival of endodontically treated premolars. J Dent Res
2007;86:729-734
(9) Esposito M1, Grusovin MG, Coulthard P, Worthington HV. The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. International Journal of Oral and Maxillofacial Implants, 696-710
(10) Wakiaga J, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic
dental stains. Cochrane Database Syst Rev. 2004;:CD004347
(11) Gresnigt MM, Kalk W, Ozcan M. Randomized clinical trial of indirect resin composite and ceramic
veneers: up to 3-year follow-up. J Adhes Dent 2013; 10-15